
Introduction
Priapism is an unwanted painful erection of the penis, not associated with sexual desire, lasting for more than four hours.
The incidence of priapism is relatively low in most Western countries, with around 0.5 cases per 100,000 person-years reported. However, these figures will be higher in countries with a high prevalence of haemaglobinopathies, such as Sickle Cell Disease (SCD).
Classification
There are two different underlying mechanisms that cause priapism:
- High flow or non-ischaemic priapism – this is caused by unregulated cavernous arterial inflow, whereby arterial blood rapidly enters the corpus cavernosum more quickly than it can be drained
- Most often associated with trauma as an underlying cause and can be triggered by sexual stimulation
- Low flow or ischaemic priapism – this is veno-occlusive in nature, caused by blockage to the venous drainage of the corpus cavernosum
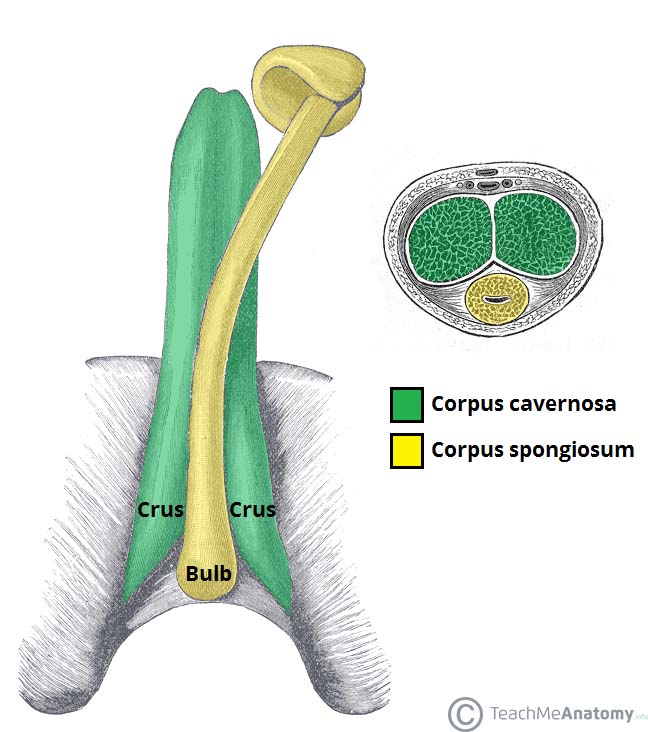
Ischaemic priapism is considered a urological emergency. Blood stays within the corpus cavernosa, although typically the glans and corpus spongiosum are unaffected.
In low flow priapism (see below), a failure of detumescence from prolonged venous stasis results in ischaemia and, if left untreated, can result in fibrosis and impotence.
Stuttering Priapism
Stuttering (also termed recurrent or intermittent) priapism is a separate condition that is characterised by repetitive and painful episodes of prolonged erections, with intervening periods of detumescence and often self-limiting.
Episodes are often shorter than in ischaemic priapism, however a single episode has the potential to progress into a major ischaemic episode. Stuttering priapism is usually expressed with patients that have SCD, with the life-long risk of priapism of a SCD patient around 29-42%.
Causes
The underlying cause of the disease determines whether high-flow or low-flow priapism. The condition is idiopathic in over half of patients.
Non-ischaemic causes are typically caused following penile or perineal trauma or spinal cord injury, whereby damage to the vasculature creates an arterial-sinusoidal shunt within the corpus cavernosum
Ischaemic causes include:
- Iatrogenic – Intracavernosal drug therapy* (for impotence), such as papaverine or alprostadil
- Sickle cell disease
- Other haematological disorders, such as leukaemia or thalassaemia
- Pelvic malignancy (rare)
*Other medication that can cause iatrogenic priapism include antipsychotics, anticoagulants, antidepressants
Clinical Features
Patients will present with an ongoing and unwanted erection that persists in the absence of sexual desires*.
In ischaemic cases, the patient presents with a painful erection and a rigid erection (hard corpus cavernosum with soft glans and spongiosum).
In cases of non-ischaemic, the erection is typically painless and the erection is not fully rigid.
*Whilst guidelines state this occurs for >4hours, most cases present (and are managed) much earlier than this
Differential Diagnosis
The diagnosis of priapism is often obvious on presentation, however the main differential is between ischaemic versus non-ischaemic.
Investigations
Following initial management (as discussed below), obtaining a corporeal blood gas will aid in initial assessment of the priapism, determining whether ischaemic or non-ischaemic (see Table 1).
| pO2 | pCO2 | pH | Lactate | |
| Ischaemic | <30mmHg | >60mmHg | <7.25 | Raised |
| Non-ischaemic | >90mmHg | <40mmHg | 7.40 | Normal |
Table 1 – Corporeal blood gas measurements for the differentiation between priapism types
Patients should have routine bloods taken which can aid in identifying the underlying cause, taken either during the acute episode or at follow-up. Bloods that should be taken include FBC, CRP and ESR, coagulation screen, bone profile, and haemoglobin electrophoresis (+/- drug screen)
In non-ischaemic cases, further work-up of any potential spinal injury may be warranted. Colour Doppler ultrasonography can also be helpful for the initial diagnosis in uncertain cases.
Management
Initial Management
The mainstay of initial management* is through corporeal aspiration, which achieves detumescence in around 30% of cases.
*Ice packs, physical exertion, and masturbation have previously been advocated as alternative conservative approaches, however are generally now deemed ineffective
Corporeal Aspiration
Corporeal aspiration is required to obtain a corporeal blood gas sample and for subsequent therapeutic benefit.
A large bore needle is inserted into the lateral edge of one corpus cavernosum. Following the diagnostic aspiration, several rounds of further aspiration and wash-out can be performed to achieve detumescence; around 10-15ml of static blood should be aspirated and replaced with normal saline until the aspirate is bright red.
If there is no response from aspiration, intracavernosal injection of a sympathomimetic agent, such as phenylephrine, may be trialled.
Surgical Management
If these manoeuvres are ineffective, a prompt surgical shunt between the corpus cavernosa and glans is fashioned.
Shunts between the erect corpora cavernosa and either the glans penis, corpus spongiosum, or saphenous vein can be attempted. This produces detumescence in around 70% of the cases, however has a common complication of subsequent erectile dysfunction.
Prognosis
Around 90% of cases with priapism lasting >24 hours do not regain the ability to have intercourse. Penile prosthesis insertion may be considered in such cases.
Key Points
- Priapism is an unwanted painful erection of the penis, not associated with sexual desire, lasting for more than one hour
- Priapism can be classified into ischaemic, non-ischaemic, and stuttering priapism
- Obtaining a corporeal blood gas will aid in initial assessment of the priapism and can be followed up by corporeal aspiration
- Around 90% of cases with priapism lasting more than 24 hours do not regain the ability to have intercourse