
Introduction
Lower urinary tract symptoms (LUTS) is a term used to describe an array of symptoms affecting the control and quality of micturition in the lower urinary tract.
LUTS can affect both men and women, although they are particularly common presentation amongst men and increase with age. It is estimated that more than 50% of men over 50 years suffer from LUTS.
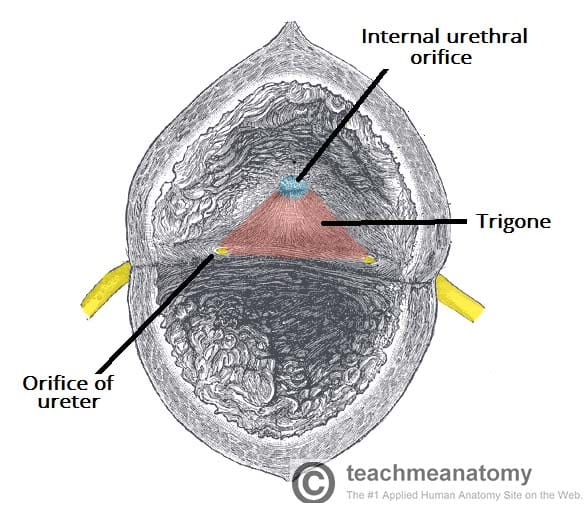
Figure 1 – The internal surface of the bladder, highlighting the trigone
Aetiology
In older men, LUTS are commonly caused by benign prostatic hyperplasia, whilst in females are most commonly associated with lower urinary tract infections
Other potential causes include bladder cancer, prostate cancer (in males), detrusor muscle weakness, pelvic floor dysfunction, chronic prostatitis, urethral stricture, from external compression e.g. pelvic tumour, and neurological disease e.g. multiple sclerosis
Lifestyle factors, including drinking fluids late at night, excess alcohol intake, and excess caffeine intake can exacerbate LUTS. Additionally, polyuria (for example secondary to diabetes mellitus, excessive fluid intake, diuretics) can exacerbate or mimic LUTS.
Classification
LUTS can be broadly categorised* into storage symptoms and voiding symptoms (Table 1):
- Storage symptoms occur when the bladder should otherwise be storing urine, therefore symptoms include urgency, frequency, nocturia, and urge incontinence
- Voiding symptoms occur usually due to bladder outlet obstruction making it more difficult to pass urine, therefore symptoms include hesitancy, intermittency, straining, terminal dribbling and incomplete emptying
|
Voiding |
Storage |
| Hesitancy or straining in micturition | Increased urinary frequency |
| Poor flow (<10mL/s) | Nocturia |
| Terminal dribble | Increased sense of urgency to urinate |
| Feeling of incomplete emptying | Urge incontinence |
Table 1 – Summary of voiding and storage symptoms
*Post-micturition symptoms is a term also increasingly being used to describe post-micturition dribble and incomplete emptying
Clinical Features
When taking a history of LUTS, ensure to clarify the exact nature of lower urinary tract symptoms present, establishing whether symptoms are mostly voiding or storage as this may can aid in determining the underlying pathology.
Ask about associated symptoms, such as visible haematuria, suprapubic discomfort, or colicky pain, and their medication history, as certain medication, including anticholinergics, antihistamines and bronchodilators, are known to exacerbate LUTS
A digital rectal examination and / or examination of the external genitalia may be helpful, depending on the presentation.
The International Prostate Symptom Score can be a useful tool for assessing and monitoring the impact of LUTS on quality of life in men, both initially and throughout any treatment course
Investigations
Initial Investigations
Post-void bladder scanning and flow rate can help distinguish between causes of LUTS*, and help to quantify the severity of the condition in those presenting with voiding symptoms. A bladder diary is often useful in highlighting patterns of behaviour which may be contributing to symptoms.
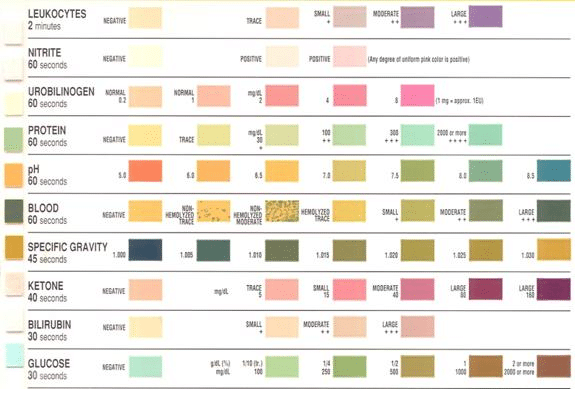
Urinalysis (Fig. 2) is usually one of the first investigations to be undertaken, assessing for signs of UTI predominantly, however also haematuria (e.g. bladder stones) or glycosuria (e.g. diabetes mellitus) may also aid in initial investigations. Urine culture should be sent to further investigate infection if relevant.
Routine blood tests, including FBC and U&Es, are useful as part of a baseline assessment, particularly if there is clinical suspicion of renal impairment or infection. Prostate-Specific Antigen (PSA) may be useful (after appropriate counselling) if there is clinical suspicion of prostatic pathology.
*For example, in overactive bladder there will be a low post-void residual, whereas in BPH there will may be high post-void residual with a flow rate low
Specialist Investigations
Urodynamic studies (Fig. 3) can be used to assess flow rate, detrusor pressure, and storage capacity if indicated (for example, in patients where neurogenic bladder dysfunction is a differential). Urodynamics is essential in women who have failed medical treatment for an overactive bladder or stress urinary incontinence and are being considered for more invasive treatment options.
Cystoscopy is the gold standard investigation for assessing the lower urinary tract and may be offered if clinically indicated, such as a history of recurrent infection or the presence of haematuria.
Upper urinary tract imaging, such as via ultrasound or CT scanning, may be useful if there is a history of chronic retention, history of recurrent infection, or the presence of haematuria.

Figure 3 – Urodynamic studies, showing a patient with potential detrusor sphincter dysynergia
Management
Conservative Management
Initial management is usually treatment of the underlying pathology. However, there are a number of conservative measures that may be useful in the initial management of LUTS in some patients whilst investigation of the underlying cause is ongoing.
Regulating fluid intake, such as timing and volume of drinks consumed and reducing caffeinated and alcoholic beverages in evenings, is important for all patients.
Individuals suffering from voiding symptoms may benefit from urethral milking techniques* (manually emptying the bulbar urethra of residual urine) or double voiding (passing urine and then remaining for a short time before passing urine again)
Pelvic floor exercises to strengthen the pelvic floor are useful in cases of stress incontinence or post-micturition dribble.
Bladder training techniques, which aim to increase the duration between the urge to void and micturition, when done properly (under supervision) these may be useful in overactive bladder.
*Particularly useful in men with significant post-micturition dribble
Pharmacological Management
Pharmacological therapies can be offered to patients in whom conservative measures are insufficient or inappropriate. The recommended pharmacological management is depends on symptomatology and underlying pathology, examples include:
- Anticholinergics (e.g. oxybutynin, tolterodine) for overactive bladder, helping to relax bladder muscle by opposing parasympathetic cholinergic control of contraction
- Mirabegron, a β3 adrenergic agonist, may also be useful in managing overactive symptoms
- Alpha blockers (e.g. alfuzosin, tamsulosin) and / or 5α-reductase inhibitors (e.g. finasteride) for BPH can help in reducing prostate size by relaxing prostatic muscle
- Loop diuretics (e.g. furosemide, bumetanide), though unlicensed, may be taken mid-afternoon to prevent nocturia
- Desmopressin is also unlicensed but has been shown to aid in reducing nocturia
Complications
Patients who retain urine post-micturition are at increased risk of infection and formation of renal and bladder calculi due to stagnation of urine.
Chronic obstruction may lead to bladder wall muscle hypertrophy or distention which can lead to overflow incontinence. Renal complications include renal failure and bilateral hydronephrosis. Acute urinary retention may also occur in patients with progressive BPH.
Key Points
- Lower urinary tract symptoms (LUTS) are a common presentation to primary and secondary care, affecting both men and women
- LUTS in men are most commonly due to benign prostatic enlargement, whereas in women they are most commonly caused by urinary tract infection
- The International Prostate Symptom Score is a useful tool for assessing and monitoring the impact of LUTS on quality of life in men, both initially and throughout any treatment course
- Ruling out non-urological pathology that may mimic LUTS, such as polyuria secondary to diabetes mellitus, is important
- There are a range of conservative, medical, and surgical management options depending on the underlying cause

