
Introduction
A radiculopathy is a conduction block in the axons of a spinal nerve or its roots, with impact on motor axons causing weakness and on sensory axons causing paraesthesia and/or anaesthesia.
There is a distinction between radiculopathy versus radicular pain:
- Radiculopathy is a state of neurological loss and may or may not be associated with radicular pain
- Radicular pain is pain deriving from damage or irritation of the spinal nerve tissue, particularly the dorsal root ganglion
In this article, we shall look at the pathophysiology, clinical features and management of radiculopathy
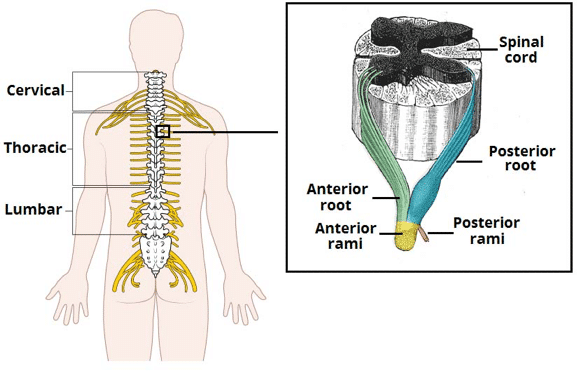
Figure 1 – The origin of the spinal nerves from the spinal cord
Aetiology
The anterior and posterior roots of the spinal nerves unite within the intervertebral foramina (Fig. 1). Both roots originate from the cord and pass to their appropriate intervertebral foramina, where each evaginates the dura mater separately before uniting to form the mixed spinal nerve.
Radiculopathy is most commonly a result of nerve compression, which can be caused by:
- Intervertebral disc prolapse
- The lumbar spine is predominantly affected by repeated minor stresses that predispose to rupture of the annulus fibrosus and sequestration of disc material (the nucleus pulposus), Fig. 2
- Degenerative diseases of the spine, including spinal canal stenosis
- The cervical spine is the most mobile segment of the spine and degenerative change is a normal part of ageing process; 80% of the population over 55 years old have degenerative changes between C5/6 and C6/7
- Fracture – either trauma or pathological
- Malignancy – most commonly metastatic
- Infection – such as extradural abscess or osteomyelitis (most commonly tuberculosis (‘Pott’s disease’))

Figure 2 – Schematic of intervertebral disc prolapse, impinging on exiting spinal nerve root
Clinical Features
Clinical features of radiculopathy include sensory features (paraesthesia and numbness) and motor features (weakness). Radicular pain is often also present, typically described as a burning, deep, strap-like, or narrow pain, it is not uncommon for the radicular pain to be intermittent.
Certain “red flag” symptoms* (Table 1) should also be specifically asked in patients with this presenting symptom, as they may indicate emergency or sinister pathology.
On examination, it is important to identify dermatomal and myotomal involvement. Ensure to evaluate for cauda equina syndrome, by assessing for pinprick sensation in the perianal dermatomes (reduced in CES), anocutaneous reflex (diminished or absent in CES), or anal tone (reduced in CES).
*It is paramount (both clinically and medico-legally) that all of these features are specifically identified, documented, and acted upon appropriately
| Red Flag | Associated Disorder |
|
Cauda Equina Syndrome (CES) |
|
Infection |
|
Fracture or infection |
|
Fracture |
|
Malignancy |
|
Metastatic disease |
Table 1 – Red Flags to clarify with any case of radiculopathy
Differential Diagnosis
The differential diagnosis for radicular pain should include pseudoradicular pain syndromes: these are conditions that do not arise directly from nerve root dysfunction, but cause radiating limb pain in an approximate radicular pattern.
These include:
- Referred pain – for example, into the arm from myocardial ischaemia, the right shoulder from hepatobiliary disease, or the flank, groin, or thigh from urinary tract
- Myofascial pain – hip muscles can mimic pain from lumbar radiculopathy; shoulder girdle muscles can produce pain radiating into the upper extremity; examine for tenderness at specific muscle sites which when palpated produce radiating pain
- Thoracic outlet syndrome – compression or irritation of the structures between the base of the neck and axilla due to anatomical variations
- Greater trochanteric bursitis – usually palpation will reveal the area of inflammation, typically over the superolateral aspect of the trochanter
- Iliotibial band syndrome – excessive friction (long distance runners, cyclists) between the iliotibial band and underlying bursa; often associated with tightness of the iliotibial tract; pain felt laterally, 2-3cm proximal to the knee joint
- Meralgia paraesthetica – compression of the lateral cutaneous nerve of the thigh as it passes under the inguinal ligament. It presents with clearly demarcated area of paraesthesia and/or numbness in the anterolateral aspect of the thigh
- Piriformis syndrome – anatomic variations in either the muscle or the sciatic nerve that can cause pain in the region of the sacroiliac joint or the sciatic notch
Investigations
The majority of cases can be diagnosed through history and clinical examination alone. However, in cases of clinical equipoise, nerve conduction studies (NCS) and / or electromyography (EMG) may be required.
Management
Definitive long-term management depends on the underlying cause. In general, the only condition that requires emergency surgical treatment is cauda equina syndrome.
Most patients with intervertebral disc prolapse an be managed non-operatively, but indications for surgical treatment include unremitting pain despite comprehensive non-surgical management, progressive weakness, and new or progressive myelopathy (compression of the spinal cord).
Symptomatic Management
Analgesia is an important aspect of management in these patients. The WHO analgesic ladder can be utilised in the first instance, however neuropathic pain medications are frequently utilised.
Amitriptyline is usually first line, or pregabalin and gabapentin as alternatives. The patients may also suffer from muscle spasms and these can be managed with benzodiazepines (often diazepam) or baclofen.
Physiotherapy remains an important part of management in this patient group.
Key Points
- Radiculopathy is the conduction block of the axons of a spinal nerve or its roots
- It presents with motor or sensory features, often also associated with radicular pain
- Ensure to enquire about specific red flag clinical features
- Radiculopathy is most commonly a result of nerve compression, which can be caused by a wide range of pathology
- Definitive long-term management depends on the underlying cause, however ensure adequate neuropathic analgesics are prescribed