
Introduction
Radial head fractures represent the most common fracture of the elbow.
They account for approximately one third of all elbow fractures, and have highest incidence in those between 20-60 years of age, with a slightly higher frequency in females.
In this article, we will look at the pathophysiology, clinical features, investigations and management of radial head fractures.
Pathophysiology
At the elbow, the radial head articulates with the capitulum of the humerus and the proximal ulna. This arrangement allows for flexion-extension and supination-pronation of the elbow.
Radial head fractures typically occur via indirect trauma; with axial loading of the forearm causing the radial head to be pushed against the capitulum of the humerus. This most commonly occurs with the arm in extension and pronation.
There are complex ligament structures that can also be damaged in these injuries, which may need further clinical/imaging assessment.
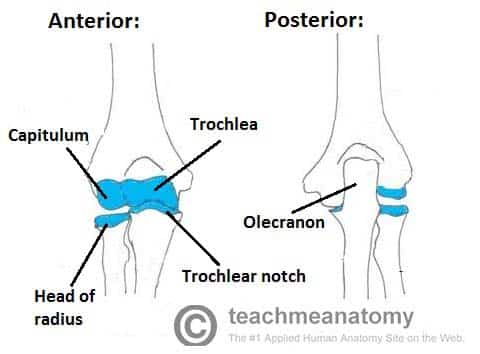
Figure 1 – Anterior and posterior views of the articulations of the elbow joint
Clinical Features
Radial head fractures often present with a history of falling on an outstretched hand followed by elbow pain. The patient may report variable degrees of swelling and bruising at the elbow.
On examination, there may be tenderness on palpation over the lateral aspect of elbow and radial head, with pain and crepitation on supination and pronation. Other clinical features include elbow effusion or limited supination and pronation movements.
Other injuries associated with a fall on an outstretched hand include wrist ligament and bony injuries*, and radial head dislocation. Therefore, the shoulder and wrist joints should always be examined.
*An Essex-Lopresti fracture describes a fracture of the radial head with disruption of the distal radio-ulnar joint, and will always require surgical intervention
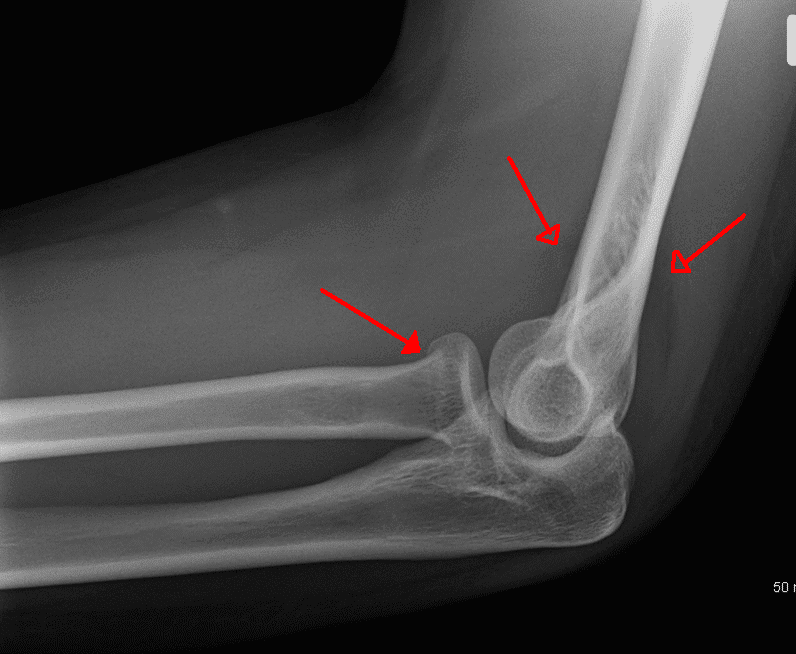
Figure 2 – Plain film radiograph of radial head fracture, with associated sail sign
Investigations
All patients presenting with suspected radial head fractures require routine blood tests, including a clotting screen and a Group and Save.
Plain antero-posterior and lateral radiographs of the elbow are required as initial imaging (Fig 2). This should including the joints above and below, if their involvement is suspected.
Radial head fractures can be easily missed on plain radiographs and occasionally only an elbow effusion may be seen. Elbow effusions on a lateral projection are termed “Sail sign”, whereby there is an elevation of the anterior fat pad, suggestive of an underlying fracture
CT imaging can be useful in evaluating more complex injuries and degree of comminution (Fig. 3). MRI imaging can be used to assess suspected associated ligament injuries.
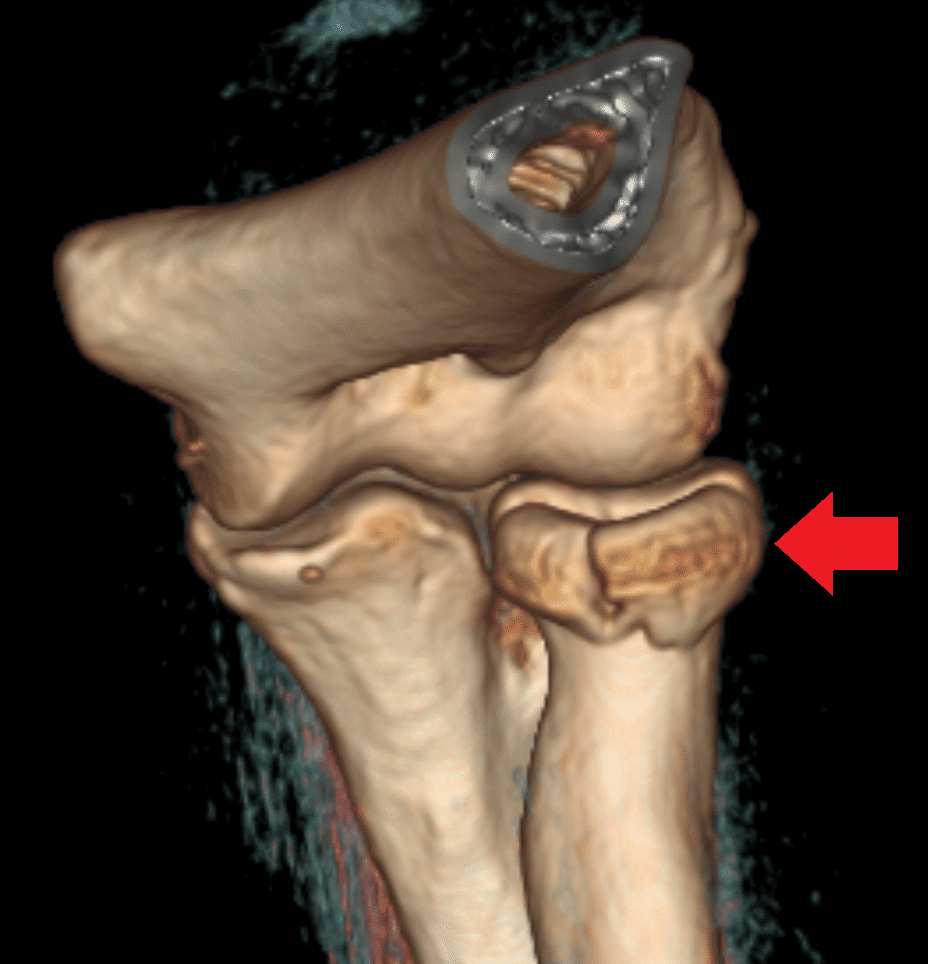
Figure 3 – A radial head fracture seen on 3D-CT reconstruction
Classification of Radial Head Fractures
Radial head fractures are classified according to the degree of displacement and intra-articular involvement, using the Mason classification:
- Mason Type 1 – Non-displaced or minimally displaced fracture (<2mm)
- Mason Type 2 – Partial articular fracture with displacement >2mm or angulation
- Mason Type 3 – Comminuted fracture and displacement (a complete articular fracture)
Management
For any patient presenting with trauma, ensure a full A to E assessment is made and resuscitated as required, prior to any definitive assessment and management of the fracture. Ensure to check the neurovascular status of the affected limb and make sure to provide adequate analgesia.
Treatment is guided by the severity of the fracture, such as that determined by the Mason classification:
- Mason type 1 – treated non-operatively, with a short period of immobilisation with sling (less than 1 week) followed by early mobilisation
- Mason Type 2 – if no mechanical block then can be treated as per a type 1 injury; if a mechanical block is present, then may need surgical intervention (typically an open reduction internal fixation, ORIF)
- Mason Type 3 – will nearly always warrant surgical intervention, either via ORIF or radial head excision or replacement (especially in highly comminuted fractures)
Patients can expect a good prognosis following a radial head fracture, however secondary osteoarthritic changes may be encountered years later, especially with fractures involving the joint surface
Key Points
- Fractures of the radial head are the most common fractures at the elbow
- Commonly occur following a fall on an outstretched hand
- Plain film radiographs are the initial investigation of choice, with both antero-posterior and lateral views
- Fracture classification is typically via the Mason classification and can help guide definitive management