Introduction
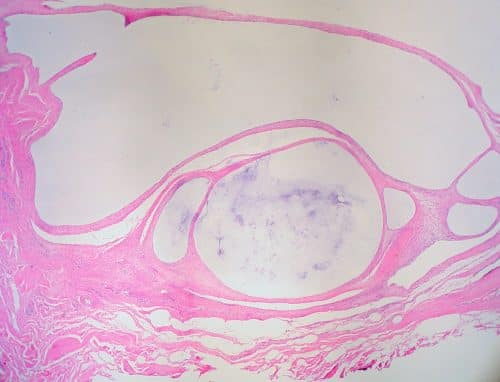
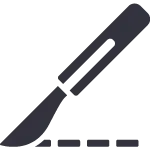
Ganglionic cysts (often termed ganglions) are non-cancerous soft tissue lumps that occur along any joint or tendon. They arise from degeneration of the joint capsule or tendon sheath of the joint, causing an outpouching filled with synovial fluid (Fig. 1).
They are most commonly found around the hands and feet, with 60-70% of ganglions appearing on the dorsal aspect of the wrist. More common in females, they have a peak age of onset of 20-40 years old.
In this article, we shall look at the risk factors, clinical features and management of ganglionic cysts.
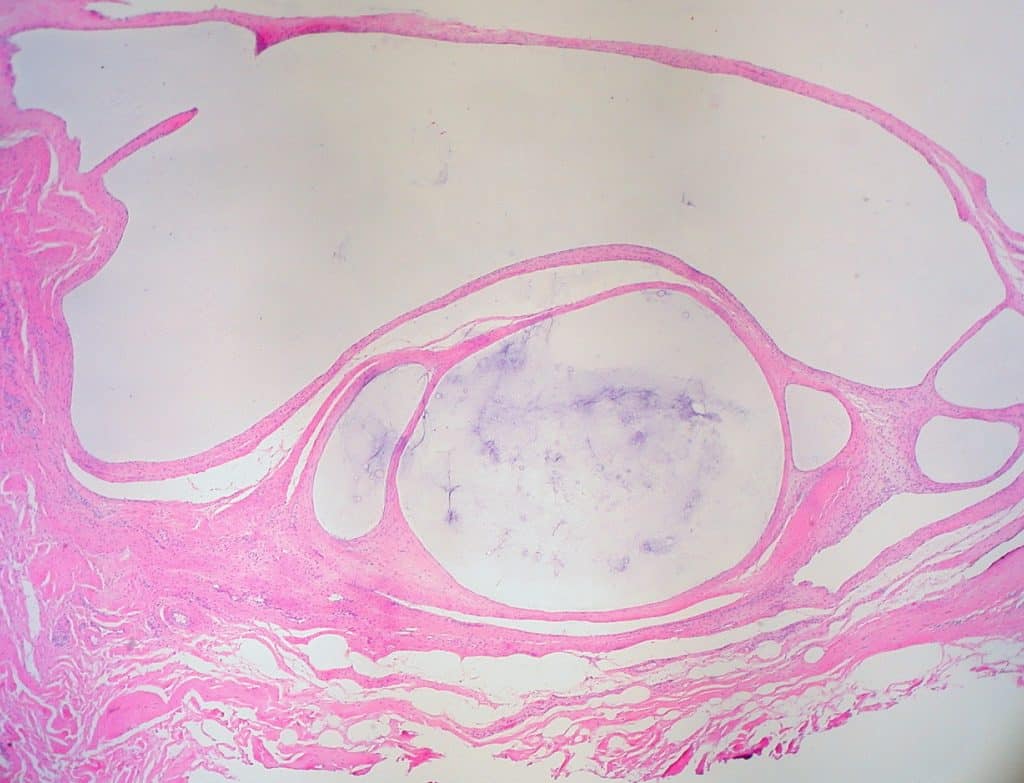
Figure 1 – Histological section of ganglionic cyst
Risk Factors
The main risk factors for developing a ganglionic cyst include female gender, the presence of osteoarthritis at the affected joint*, or previous joint or tendon injury
*Osteoarthritis can cause an increase of the fluid in the joint, resulting in a leakage through the tendon sheath into the cyst
Clinical Features
A ganglionic cyst typically presents as a smooth spherical painless lump adjacent to the joint affected (Fig. 2). It may have appeared suddenly or grown over time; in some cases, the cyst may have subsided initially, to then reappear at a later date.
On examination of the hand, the lump will be soft and will transilluminate, however may mechanically restrict the full range of motion in the affected joint.
If the cyst exerts any pressure upon an adjacent nerve(s), the patient may present with localised paresthesia, pain, or motor weakness.
Figure 2 – (A) Ganglion located on the volar aspect of the wrist (B) Ganglion located on the dorsal surface of the hand
Differential Diagnosis
The main differentials to consider include:
- Lipoma – This will not be entirely spherical and does not trans-illuminate
- Osteoarthritis – usually accompanied from a long standing osteoarthritis of the scaphotrapeziotrapezoid joint, presenting as a palpable, hard, non-cystic, and immobile mass that does not trans-illuminate
- Tenosynovitis– swelling presents along the tendon, with no discrete mass present
- Giant cell tumour of tendon sheath – the mass is solid, does not transilluminate, and is fixed to the underlying sheath
Investigations
Most ganglion cysts can be diagnosed clinically. A plain film radiograph may assist in ruling out osteoarthritis or bone malignancies as differentials if suspected
In uncertain cases, imaging via ultrasound or MRI scan* can be done in order to assess the shape, size, and depth of the cyst.
A ganglionic cyst can be aspirated for temporary symptomatic relief (however there is a high rate of recurrence) and any fluid extracted can be sent off for microscopy +/- cytology if required.
*Due to their high sensitivity, such imaging modalities may also pick up incidental cysts that have not yet grown large enough to be symptomatic
Management
If the cyst does not cause any pain, the usual recommended treatment is to simply monitor, as cysts often disappear spontaneously without further intervention.
If the cyst causes pain or severely limits range of movement, there are two main interventions that can be performed:
- Aspiration +/- steroid injection*, although this is associated with infection and a higher rate of recurrence
- *There is only limited evidence demonstrating a clear benefit of steroid injections in ganglion
- Cyst excision, removing the cyst capsule along with a portion of the associated tendon sheath (recurrence is less than with aspiration, but still possible)
- Often reserved for symptomatic cases with recurrence following aspiration
Key Points
- Ganglionic cysts are non-cancerous soft tissue lumps that occur along any joint or tendon
- They appear as smooth spherical painless lumps, that are soft and transilluminate on examination
- Diagnosis is clinical and most cases will be managed conservatively, intervention only indicated in symptomatic cases or those limiting range of movement